
Effect of empathy and win-win psychological intervention on nursing of patients with acute cerebral infarction based on psychological stress and coping styles
Vliv empatie a psychologické intervence win-win na ošetřovatelskou péči o pacienty s akutním mozkovým infarktem v důsledku psychického stresu a vliv různých způsobů zvládání stresu
Východiska: Akutní mozkový infarkt (acute cerebral infarction; ACI) je časté cerebrovaskulární onemocnění charakterizované akutním nástupem a závažným stavem. Cíl: Naším cílem bylo posoudit vliv empatie a psychologické intervence win-win na ošetřovatelskou péči o pacienty s ACI v důsledku psychického stresu a vliv různých způsobů zvládání stresu. Metody: Pacienti s ACI (n = 50), kteří byli od června 2021 do prosince 2022 podrobeni rutinní ošetřovatelské intervenci, byli zařazeni do kontrolní skupiny, zatímco pacienti (n = 50), kteří byli od ledna 2023 do června 2024 podrobeni rutinní ošetřovatelské intervenci kombinované s empatií a psychickou intervencí win-win, byli zařazeni do studijní skupiny. Výsledky: Studijní skupina měla vyšší skóre v dimenzi konfrontace, ale nižší skóre v dimenzích vyhýbání se a rezignace než kontrolní skupina (p < 0,05). Skóre General Self-Efficacy Scale (GSES) se zvýšilo, zatímco skóre Fear of Progression Questionnaire-Short Form (FoP-Q-SF) se snížilo ve srovnání s hodnotami před intervencí v obou skupinách. Studijní skupina měla vyšší skóre GSES, ale nižší skóre FoP-Q-SF než kontrolní skupina (p < 0,05). Skóre Stroke-Specific Quality of Life Scale se v obou skupinách zvýšilo ve srovnání s hodnotami před intervencí (p < 0,05). Závěr: Empatie a psychologická intervence win-win mohou zmírnit psychický stres pacientů s ACI a jejich příbuzných a zlepšit způsoby, jak pacienti zvládají situaci.
Klíčová slova:
stres – ošetřovatelství – empatie – akutní mozkový infarkt – zvládání stresu – psychologická intervence
Authors:
W. Bian; N. Zhu; F. Gu; L. Ding; J. Zhang; J. Yu; Y. Hu
Authors place of work:
Department of Emergency, Jiangnan University Affiliated Hospital, Wuxi, Jiangsu Province, China
Published in the journal:
Cesk Slov Neurol N 2025; 88(3): 183-188
Category:
Původní práce
doi:
https://doi.org/10.48095/cccsnn2025183
Summary
Background: Acute cerebral infarction (ACI) is a common cerebrovascular disease characterized by acute onset and severe condition. Aim: We aimed to assess the effect of empathy and win - -win psychological intervention on the nursing of patients with ACI based on psychological stress and coping styles. Methods: ACI patients (N = 50) who were given routine nursing intervention from June 2021 to December 2022 were enrolled as a control group, while patients (N = 50) who were given routine nursing intervention combined with empathy and win-win psychological intervention from January 2023 to June 2024 were enrolled as a study group. Results: The study group had a higher score in the confrontation dimension, but lower scores in the avoidance and resignation dimensions than those from the control group (P < 0.05). The General Self-Efficacy Scale (GSES) score increased, while the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) score decreased in both groups compared with those before intervention. The study group had a higher GSES score, but a lower FoP-Q-SF score than those from the control group (P < 0.05). The Stroke-Specific Quality of Life Scale score increased in both groups compared with that before intervention (P < 0.05). Conclusion: Empathy and win-win psychological intervention can alleviate the psychological stress in ACI patients and their relatives, improve patients‘ coping styles.
Keywords:
nursing – stress – Coping – empathy – acute cerebral infarction – psychological intervention
Introduction
Acute cerebral infarction (ACI), a common cerebrovascular disease characterized by acute onset and severe condition, is defined as ischemic necrosis or softening of brain tissues caused by cerebral blood circulation disorders, presenting with acute neurological deficits [1]. Intravenous thrombolysis and thrombectomy following prompt hospitalization can save the life of ACI patients, but a series of sequelae, such as physical dysfunction and motor dysfunction, may affect most patients postoperatively. In this state, patients may experience certain psychological pressure, worsening psychological stress. As a result, they will select a negative coping style in treatment or rehabilitation training, seriously harming the prognosis [2,3]. Targeted nursing intervention during treatment and rehabilitation has positive significance in promoting postoperative functional recovery of ACI patients [4,5]. Empathy and win-win psychological intervention based on psychological stress and coping styles is a nursing intervention mode that can help patients adapt to disease and rehabilitation process by evaluating patients‘ psychological stress sources and coping mechanisms, and then taking corresponding intervention measures that can enhance nursing staff-patient understanding and emotional resonance.
At present, few reports are available about the application of this intervention mode in ACI. In view of this, the effect of empathy and win-win psychological intervention based on psychological stress and coping styles in the nursing of ACI patients was assessed in this study.
Materials and methods
Subjects
Acute cerebral infarction patients (N = 50) who were given routine nursing intervention from June 2021 to December 2022 were enrolled as a control group, while patients (N = 50) who were given routine nursing intervention combined with empathy and win-win psychological intervention from January 2023 to June 2024 were enrolled as a study group. To assess the baseline level of self-sufficiency, the Barthel Index [6] was used upon admission. This scale evaluates activities of daily living such as feeding, bathing, dressing, mobility, and continence, with a total score ranging from 0 (completely dependent) to 100 (completely independent). Patients with a Barthel Index score ≥ 60 were considered to have moderate-to-good self-sufficiency, while those scoring < 60 were classified as having low self-sufficiency. The general data were comparable between the two groups (P > 0.05) (Tab. 1).
Inclusion and exclusion criteria
Inclusion criteria were as follows:
a)
patients meeting the diagnostic criteria for ACI [7];
b) those with complete clinical data;
c)
those with clear consciousness and stable conditions;
d) those with first-episode ACI;
e)
those whose caregivers were older than 18 years and could be responsible for the patient‘s primary nursing and medical decision-making.
Exclusion criteria included:
a)
patients who or whose primary caregivers were unable to fill in the scale due to mental disorders/communication disorders;
b)
those who were transferred to another hospital or died halfway;
c)
those complicated with severe respiratory or immune system diseases or malignancies;
d)
those complicated with coagulation disorders or other cardio-cerebrovascular diseases;
e)
those with dysfunction/failure of vital organs;
f)
those whose relatives intended to give up treatment.
Intervention method for the control group
Routine nursing intervention was adopted, including distributing brochures, strengthening communication with patients and their families, conducting oral education and guidance on sleep, diet, and exercise, comforting patients with adverse emotions by using words, and instructing patients to use drugs according to the doctor‘s advice.
Intervention method for the study group
Routine nursing intervention (same as the control group) combined with empathy and win-win psychological intervention were adopted:
1.
Establishment of an empathy and win-win psychological intervention team: All members regularly received relevant training and learning about communication skills, empathy theory, psychology and humanistic care, and they could take up their posts only after passing the examination.
2.
Assessment of patient data: The patient data (age, personality characteristics, educational level, occupation, etc.) was collected by medical record forms, observation, communication, listening, etc.
3.
Implementation of nursing intervention:
a)
The nursing staff patiently listened to patients‘ appeal and checked their family and cultural backgrounds to fully grasp their personality characteristics and physiological and psychological feelings, communicated with patients in a transpositional way, and analyzed the main factors causing patients‘ psychological stress (family support, social environment, external substances, etc.).
b)
The nursing staff assisted patients and their family members in developing a habit of keeping rehabilitation diaries, informed family members of the recent improvement in patients‘ conditions by asking questions, guided family members to express sufficient support willingness, helped patients recall past struggle and brilliant moments, understood and guided patients to talk about pain, and gave affirmation and approval.
c)
The nursing staff provided teaching videos of psychological education and ACI health knowledge for patients and their relatives, instructed patients and their relatives to take relaxation training such as meditation, deep breathing, and music therapy, and played soothing and soft piano music every day.
d)
The nursing staff informed relatives of the treatment expenses in a timely manner. Charity funds could be established to offer various economic relief channels for families with financial difficulties.
4.
Out-of-hospital continuous psychological intervention: A WeChat group for ACI rehabilitation training was created to regularly share the benefits or teaching videos of rehabilitation exercise, relaxation training, and emotional resolution as well as treatment rehabilitation cases with patients and their relatives, ask questions every day, and encourage patient/family members to actively answer and discuss. Moreover, patients and their relatives were encouraged to actively participate in friend and community activities, patient exchange meetings were organized twice a month, and patients with better recovery were invited to share their experiences in the recovery process.

Outcome measures
The following indicators were evaluated before intervention and at 8 weeks of intervention:
1.
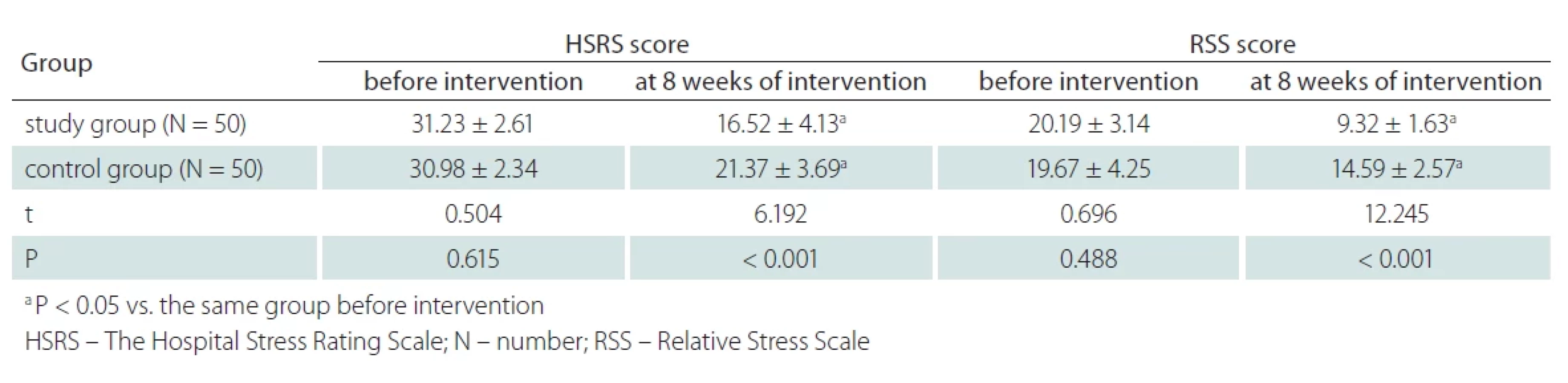
Psychological stress levels of patients and their relatives: The Hospital Stress Rating Scale (HSRS) prepared by Volicer and Bohannon was used to evaluate the psychological stress level of patients in the two groups [6]. HSRS covered 49 items in 5 dimensions (lack of confidence, unfamiliar environment, disease threat, family social factors, and discomfort). Each item was scored 0 or 1 point (no = 0, yes = 1), and the total score was 0–49 points. The lower the score, the lower the psychological stress level of patients. Besides, the Relative Stress Scale (RSS) was used to evaluate the psychological stress level of relatives (primary caregivers) in the two groups [9]. RSS was composed of 15 items in 3 dimensions, i.e., the degree of disturbance in life (5 items), the psychological pain experienced (6 items), and the degree of negative emotion (4 items). Each item was scored 0–2 points, and the total score was 0–30 points. A higher score signifies a higher psychological stress level of relatives.
2.
Patients‘ coping styles: The Medical Coping Modes Questionnaire (MCMQ) was used to evaluate the patients‘ coping styles in the two groups [10]. MCMQ was composed of 20 items in 3 dimensions, i.e., confrontation (8 items: 4 scored forwardly and 4 scored reversely), avoidance (7 items: 5 scored forwardly and 2 scored reversely), and resignation (5 items: 2 scored forwardly and 3 scored reversely). Each item was scored 1–4 points. The higher the score of each dimension, the more likely the patients were to choose this coping style.
3.
Patients‘ self-efficacy and fear of disease: The General Self-Efficacy Scale (GSES) was adopted to evaluate self-efficacy [11]. GSES consisted of 10 items, and each item was scored 1–4 points according to the answer. The total score was 10–40 points, and a higher score corresponded to stronger self-confidence and self-efficacy. Besides, the patients‘ fear of disease was evaluated using the Fear of Progression Questionnaire-Short Form (FoP-Q--SF) [12]. FoP-Q-SF included 12 items, and each item was scored 1–5 points according to the answer (never, rarely, sometimes, often, and always). The total score was 12–60 points, and the lower the score, the less the fear.
4.
Quality of life (QoL) of patients: QoL was evaluated using the Stroke-Specific Quality of Life Scale (SS-QOL) [13]. It covered 49 items in 12 dimensions (family role, physical fitness, vision, mobility, emotion, language, etc.). Each item was scored 1–5 points according to the answer (completely yes, basically yes, uncertain, basically no, and completely no). The total score was 245 points, and a higher score corresponded to higher QoL.
Statistical analysis
SPSS 23.0 (IBM, Armonk, NY, USA) software was used for the statistical analysis. Measurement data were described by mean ± standard deviation (x – ± s) and subjected to the t-test. Count data were described by percentage (N [%]) and subjected to the c2 test. P < 0.05 was considered statistically significant.
Results
Baseline clinical data
Baseline clinical data were comparable between the two groups (P > 0.05) (Tab. 1).
Psychological stress levels of patients and their relatives
At 8 weeks of intervention, the scores of HSRS and RSS declined in both groups compared with those before intervention, and they were lower in the study group than in the control group (P < 0.05) (Tab. 2).
Patients‘ coping styles
At 8 weeks of intervention, the scores of MCMQ in the confrontation dimension increased, while the scores in the avoidance and resignation dimensions decreased in both groups compared with those before intervention. Moreover, the study group had a higher score in the confrontation dimension, but lower scores in the avoidance and resignation dimensions than in the control group (P < 0.05) (Tab. 3).

Patients‘ self-efficacy and fear of disease
At 8 weeks of intervention, the GSES score increased, while the FoP-Q-SF score decreased in both groups compared with those before intervention. Moreover, the study group had a higher GSES score, and a lower FoP-Q-SF score than the control group (P < 0.05) (Tab. 4).

Patients‘ QoL
At 8 weeks of intervention, the SS-QOL score increased in both groups compared with that before intervention, and it was higher in the study group than in the control group (P < 0.05) (Tab. 5).

Discussion
As demonstrated by recent studies, stroke has become the second leading cause of death worldwide, and ACI is the major type of stroke, accounting for about 70–80% [14]. Although interventional therapy for ACI has a high success rate, the disability rate is high, and the postoperative rehabilitation process is slow. As the primary caregivers of patients, patients‘ relatives need to not only worry about disease progression, but also bear the burden of care and budget [15,16]. In addition, patients‘ relatives have no time to adapt to the new role as caregivers due to the acute onset of ACI, resulting in a series of psychological crises for patients and their relatives [17]. Routine nursing intervention mainly focuses on health education and rehabilitation guidance within hospitals and lacks attention to psychological stress of patients and their families. Moreover, cognitive evaluation of different patients on stress sources varies. Therefore, it is necessary to explore targeted psychological intervention plans based on individual conditions.
Acute cerebral infarction patients need to face self-perceived burdens such as lack of self-care ability, and increased pressure on family budget and care, and their demands may vary dynamically across stages of the disease. Therefore, nursing staff must develop effective intervention measures according to the psychological changes and demands of patients at different stages, thereby providing patients with continuous guidance and support and helping patients maintain a positive attitude toward psychological rehabilitation [18–20]. In this study, HSRS, FoP-Q-SF, and RSS scores were lower in the study group than in the control group at 8 weeks of intervention, suggesting that empathy and win-win psychological intervention can relieve the psychological stress of ACI patients and their relatives and reduce their fear of ACI. The reason is that in the empathy and win-win psychological intervention, nursing staff should be trained with empathy ability before they can take up their posts, so that they can fully grasp the contradiction of “psychological imbalance” in patients and their relatives during nursing, thereby making decisions in empathy and win-win nursing from the perspective of empathy and sympathy, and inducing patients to actively express their inner pain to reduce psychological stress. Nursing staff should communicate with patients patiently in a transpositional way, and imagine the possible negative emotions such as psychological pressure, worry about health and anxiety regarding economic pressure they may face as patients, so that they can better understand patients‘ feelings and demand changes, thereby taking more personalized nursing measures, and helping patients better relieve feelings, cope with psychological stress and pressure brought about by ACI sequelae, and enhance motivation in rehabilitation. Nursing staff should also provide teaching videos on psychological education and ACI health knowledge for patients and their relatives, and create a WeChat group for ACI rehabilitation training, so that patients‘ relatives can accept the role change more quickly, and patients and their relatives can further analyze and understand the problems they face and learn to cope with troubles in life using psychological skills to reduce patients‘ fear of disease and ease the tension. Moreover, various economic relief channels should be offered for families with financial difficulties, and nursing staff should assist patients and their relatives in developing a habit of keeping rehabilitation diaries and recalling past struggles and brilliant moments, so that patients and their relatives can review good things in the past to alleviate psychological pressure and establish confidence in life and rehabilitation [21].
The study group had higher scores of GSES, SS-QOL, and MCMQ in the confrontation dimension, and lower scores of MCMQ in the avoidance and resignation dimensions than the control group at 8 weeks of intervention, suggesting that empathy and win-win psychological intervention based on psychological stress and coping styles can enhance both self-efficacy and QoL of ACI patients and improve their coping styles. The reason is that empathy-based communication enables nursing staff to fully enter the patients‘ inner world, makes patients feel respected, accepted, understood, and less lonely in ACI rehabilitation, fully arouses the patients‘ resonance, boosts the nurse--patient relationship, and inspires the patients‘ confidence and self-efficacy in overcoming the disease, thereby responding to ACI rehabilitation more positively. Participation in patient exchange meetings and friend and community activities can offer more opportunities for positive behavior support, emotional communication and social support, and reduce social isolation caused by ACI. Moreover, sharing the experiences of patients with better recovery can stimulate patients‘ confidence in recovery, improving self-efficacy such as disease management [22]. In summary, by increasing the accuracy of perceiving ACI patients‘ psychological changes, empathy and win - -win psychological intervention can help patients re-establish confidence in life, thereby achieving the goal of nursing-patient empathy and win-win.
Conclusion
In conclusion, empathy and win-win psychological intervention can alleviate the psychological stress of ACI patients and their relatives, improve patients‘ coping styles, reduce their fear of ACI, and enhance their self--efficacy and QoL, which is worthy of application and popularization in clinical nursing.
Ethics approval and consent to participate
The entire study was conducted in accordance with the Helsinki Declaration of 1975 (as revised in 2004 and 2008). The study has received ethical approval by Jiangnan University Affiliated Hospital (No. LS2021097, 5. 6. 2021). All participants signed a written informed consent to participate in the study. All methods in the presented study were performed in accordance with relevant guidelines and regulations.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors‘ contributions
W.B. designed the study, N.Z. conceived and supervised the study, F.G. and L.D. performed and analyzed the experiments, and J.Z. and Y.H. drafted the paper.
Conflict of interest
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
Zdroje
1. Mao X, Luan D, Qi Z. Dysregulation of Serum miR-138-5p and its clinical significance in patients with acute cerebral infarction. Cerebrovasc Dis 2022; 51 (5): 670–677. doi: 10.1159/000523902.
2. Xie H, Gao M, Lin Y et al. An emergency nursing and monitoring procedure on cognitive impairment and neurological function recovery in patients with acute cerebral infarction. NeuroRehabilitation 2022; 51 (1): 161–170. doi: 10.3233/NRE-210310.
3. Song TJ, Chang Y, Chun MY et al. High dietary glycemic load is associated with poor functional outcome in patients with acute cerebral infarction. J Clin Neurol 2018; 14 (2): 165–173. doi: 10.3988/jcn.2018.14.2.165.
4. Liu Y, Qu M, Wang N et al. Effects of an evidence-based nursing intervention on neurological function and serum inflammatory cytokines in patients with acute cerebral infarction: a randomized controlled trial. Restor Neurol Neurosci 2021; 39 (2): 129–137. doi: 10.3233/RNN-201080.
5. An X, Zeng L, Shen L et al. Influences of a hierarchical nursing model on rescue outcomes and nursing quality of patients with acute cerebral infarction. Am J Transl Res 2021; 13 (6): 6498–6506.
6. Martín Moreno V, Martínez Sanz MI, Fernández Gallardo M et al. The influence of nationwide COVID-19 lockdown on the functional impairment and long-term survival of dependent people for carrying out basic activities of daily living in a neighborhood of the city of Madrid, Spain: Orcasitas Cohort Longitudinal Study. Front Public Health 2024; 12 : 1385058. doi: 10.3389/fpubh.2024.1385058.
7. Hacke W, Kaste M, Skyhoj Olsen T et al. Acute treatment of ischemic stroke European Stroke Initiative (EUSI). Cerebrovasc Dis 2000; 10 (3): 22–33. doi: 10.1159/000047578.
8. Volicer BJ, Bohannon MW. A hospital stress rating scale. Nurs Res 1975; 24 (5): 352–359.
9. Thommessen B, Aarsland D, Braekhus A et al. The psychosocial burden on spouses of the elderly with stroke, dementia and Parkinson‘s disease. Int J Geriatr Psychiatry 2002; 17 (1): 78–84. doi: 10.1002/ gps.524.
10. Chai Q, Yuan Z, Jin Y et al. Factors influencing acceptance of disability among stroke patients in Tianjin, China: a cross-sectional study. NeuroRehabilitation 2016; 38 (1): 37–44. doi: 10.3233/NRE-151293.
11. Chen HL, Liu K, You QS. Self-efficacy, cancer-related fatigue, and quality of life in patients with resected lung cancer. Eur J Cancer Care 2018; 27 (6): e12934. doi: 10.1111/ecc.12934.
12. Sarkar S, Sautier L, Schilling G et al. Anxiety and fear of cancer recurrence and its association with supportive care needs and health-care service utilization in cancer patients. J Cancer Surviv 2015; 9 (4): 567–575. doi: 10.1007/s11764-015-0434-2.
13. Legris N, Devilliers H, Daumas A et al. French validation of the Stroke Specific Quality of Life Scale (SS-QoL). NeuroRehabilitation 2018; 42 (1): 17–27. doi: 10.3233/NRE-172178.
14. Zhu FX, Ye Q. Effect of medical care linkage-continuous management mode in patients with posterior circulation cerebral infarction undergoing endovascular interventional therapy. World J Clin Cases 2022; 10 (29): 10478–10486. doi: 10.12998/wjcc.v10.i29.10478.
15. Pego Pérez ER, Fernández I, Pumar JM. Functional outcomes of patients with stroke treated with thrombectomy by aspiration. Brain Inj 2021; 35 (4): 476–483. doi: 10.1080/02699052.2021.1887519.
16. Munich SA, Vakharia K, McPheeters MJ et al. “Strokenomics”: bending the cost curve in stroke care. J Neurosurg 2020; 134 (2): 585–590. doi: 10.3171/2019.11.JNS191960.
17. Li Z, Shang N, Fan G et al. Effect of nursing based on the hopeless self-esteem theory plus multi-dimensional intensive nursing for elderly patients with acute cerebral infarction complicated with depression. Am J Transl Res 2021; 13 (7): 8450–8457.
18. Tang X, Sun H, Ge S et al. Experiences and needs of older adults at different stages of cerebral infarction based on trajectory theory-A qualitative study. Nurs Open 2023; 10 (3): 1482–1491. doi: 10.1002/ nop2.1398.
19. Onishi R, Hatakeyama Y, Hirata K et al. Development and usability of a hospital standardized ADL ratio (HSAR) for elderly patients with cerebral infarction: a retrospective observational study using administrative claim data from 2012 to 2019 in Japan. BMC Geriatr 2023; 23 (1): 235. doi: 10.1186/s12877-023-03957-4.
20. Prusova E, Skoloudik D, Langova K et al. Efekt psychoedukačního programu u pacientů s CMP v postakutní péči. Ces Slov Neurol N 2023; 86/119 (6): 383–390. doi: 10.48095/cccsnn2023383.
21. Jiang X, Gu Q, Jiang Z et al. Effect of family-centered nursing based on timing it right framework in patients with acute cerebral infarction. Am J Transl Res 2021; 13 (4): 3147–3155.
22. Chen QQ, Lin FM, Chen DH et al. Analysis of mental health status and related factors in patients with acute cerebral infarction.World J Psychiatry 2023; 13 (10): 793–802. doi: 10.5498/wjp.v13.i10.793.
Štítky
Dětská neurologie Neurochirurgie NeurologieČlánek vyšel v časopise
Česká a slovenská neurologie a neurochirurgie

2025 Číslo 3
Nejčtenější v tomto čísle
- Drug-induced changes and disorders of sleep and wake cycles – a narrative review
- Telerehabilitation in people with neurological diseases – current findings from clinical studies
- Paraneoplastic movement disorders
- Introduction to the role of hypofractionated gamma knife therapy in brain metastases