
Traumatic bilateral vertebral artery dissection
Authors:
T. Švecová 1; T. Hulínová 2,3; P. Handlos 1,4; J. Bejbl 2; H. Kolářová 5; V. Novák 6
Authors place of work:
Department of Forensic Medicine, University Hospital Ostrava, Ostrava, Czech Republic
1; Department of Clinical and Molecular, Pathology and Medical Genetics, University Hospital Ostrava, Ostrava, Czech Republic
2; Department of Clinical and Molecular, Pathology, Palacký University Olomouc, Olomouc, Czech Republic
3; Department of Intensive Medicine and, Forensic Studies, Faculty of Medicine, Ostrava University, Ostrava, Czech, Republic
4; Translation and interpreting services, Ostrava, Czech Republic
5; Department of Neurosurgery, University, Hospital Olomouc, Palacký University, Olomouc, Olomouc, Czech Republic
6
Published in the journal:
Cesk Slov Neurol N 2025; 88(4): 253-255
Category:
Dopisy redakci
doi:
https://doi.org/10.48095/cccsnn2025253
Dear Editors,
Traumatic vertebral artery injury encompasses both blunt and penetrating trauma [1]. In addition to traumatic causes, vertebral artery injuries may occur spontaneously due to vascular or connective tissue conditions. Blunt trauma to the head and neck region frequently results in vascular injury. These injuries can result in stroke or transient ischemic attacks, with the primary issue being restricted blood flow through the posterior circulation, primarily supplied by vertebral arteries. Therefore, patients may present with stroke-related symptoms, including impaired speech and swallowing, visual disturbances, and ataxia, and in severe cases, even paresis and impaired consciousness.
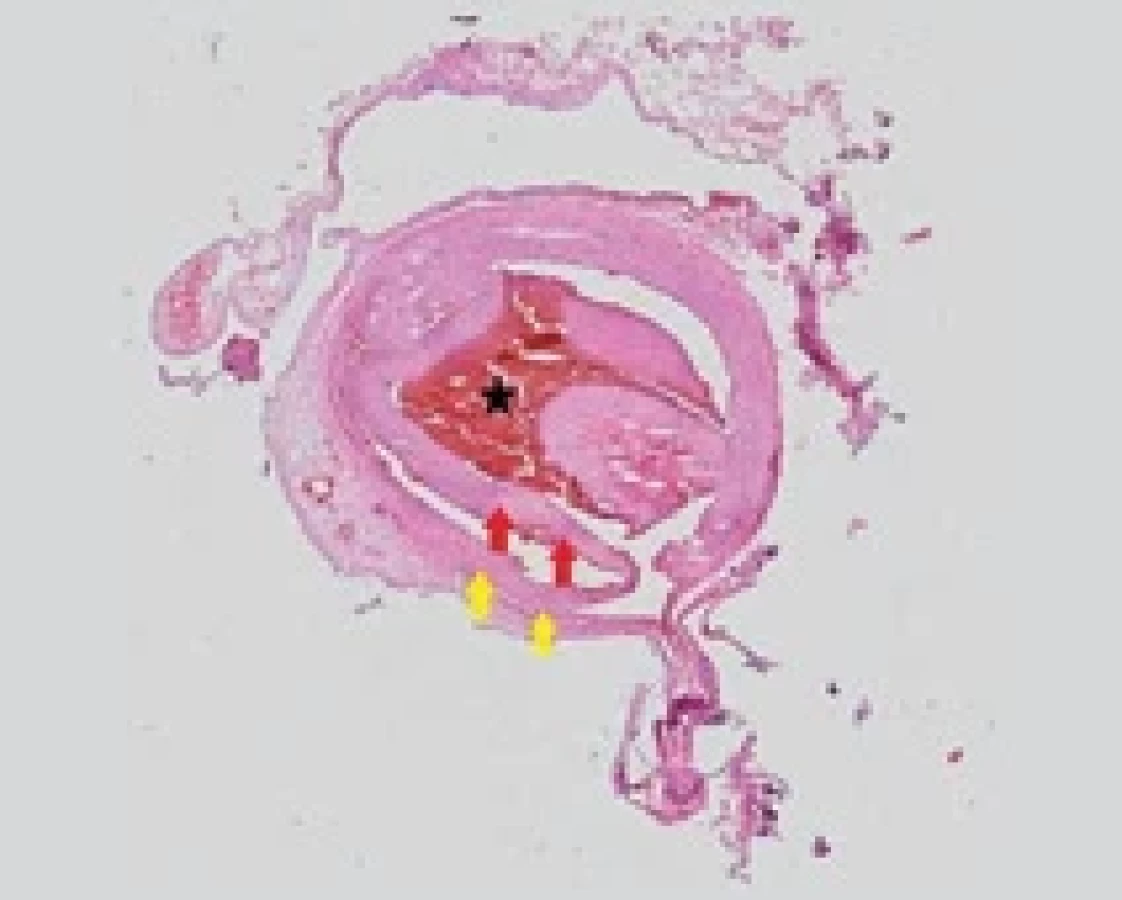
A 65-year-old male fell 5 meters down a steep slope while picking mushrooms, hitting his head on a stone, resulting in head trauma. At the scene, the patient was found unconscious, and his wife called emergency services. Upon arrival, paramedics initiated resuscitation efforts. Subsequently, the patient was airlifted to the emergency department for further care. Upon admission, the patient remained unconscious and exhibited respiratory distress, left-sided anisocoria, and hypercapnia. His limbs were pale and cold, with weak arterial pulsations. The Glasgow Coma Scale (GCS) score was 3, indicating unresponsiveness, and the patient required artificial ventilation. Following the administration of medications (Propofol, Dithiaden, Sufentanil, Noradrenaline, Rocuronium, Empressin, Cordarone, Fraxiparin, Dobuject, Albumin, Hydrocortisone, Amoxiclav), circulatory stability was temporarily restored. CT imaging revealed fractures of the spinous processes of the C4 and C5 vertebrae, soft tissue contusion of the head, bilateral pulmonary contusions, and a suspected bilateral dissection of the vertebral arteries. CTA subsequently confirmed bilateral vertebral artery dissection extending from the C3 to C5 levels, along with the presence of cerebral edema (Fig. 1 a–d). Over the next 4 days, the patient‘s condition worsened gradually, his circulatory system was unstable necessitating significant vasopressor support and analgosedation. Laboratory results indicated the development of hypernatremia and hyperchloremia. Treatment was initially focused on stabilizing the patient‘s condition with vasopressor support, therefore early endovascular intervention was not deemed due to the patient’s provisional grim prognosis. On the fifth day after admission, the patient developed multi-organ failure, oligoanuria, and severe metabolic disorder. Control CT scan revealed transtentorial and occipital conus herniation and malignant cerebral edema (Fig. 1 e, f). As the cerebral edema progressed, CT scan revealed the condition after vertebral artery bilateral dissection, bilateral occlusion, posterior basin not filled with blood intracranially, and the anterior basin only to M1–M2 and A1–A2 segment. This condition culminated in the death of the patient in a coma after six days of hospitalization. External examination of the deceased disclosed laceration-contusion wounds and skin abrasions. Internally, findings included soft tissue hemorrhage within the soft skullcaps, fractures of the C4 and C5 cervical vertebrae‘s spinous processes, bilateral vertebral artery dissection, and brain disintegration. Microscopic examination revealed a separation of a portion of the vertebral artery wall towards the lumen, accompanied by surrounding vascularity (Fig. 2). The cause of death was traumatic cerebral edema. Vertebral artery dissection, a phenomenon encountered in forensic practice, typically arises from forceful hyperextension and rotational movements, resulting in arterial tension across the cervical vertebrae and subsequent intimal tear.

Vertebral artery dissection often remains an underdiagnosed complication following cervical spine trauma, most commonly luxation, subluxation, or fractures of the cervical vertebrae or their processes [2]. The region most frequently affected along the vertebral artery‘s course is the atlantooccipital articulation area, where the artery transitions from a vertical to a horizontal orientation. Etiologically, dissections are typically categorized as spontaneous or traumatic, with consideration given to the risks associated with chiropractic interventions [3] and massage techniques, where these practices can lead to patient disability. Spontaneous dissections most commonly occur in the presence of predisposing factors (fibromuscular dysplasia, Ehler-Danlos syndrome). Symptoms of arterial injury may obscure those arising from spinal trauma and may take several hours or even days to appear [4]. In cases of lower injury severity, clinical symptoms may include headache, neck pain, nausea, vomiting, vertigo, and ataxia. Life-threatening manifestations may include paralysis or subarachnoid hemorrhage [5]. The optimal diagnostic approach involves performing brain CT, CTA, and whole-body CT to identify or rule out associated organ complications [6]. Arterial dissection results in intimal layer rupture, separation of arterial wall layers, and blood entry into the false lumen, culminating in stenosis or aneurysmal dilatation. Ischemia may arise either from stenosis of the affected feeding artery, or from distal embolization of the thrombus [7].
Based on injury severity, location, and clinical presentation of the injury, treatment modalities such as anticoagulation, antiplatelet therapy, or endovascular intervention may be employed. The current management system for blunt vertebral artery injuries advocates for forceful therapy with antithrombotic medications. This therapy aims to prevent neurologic sequelae in the posterior cerebral circulation. Anticoagulation treatment remains the most commonly employed method for managing vertebral artery injuries resulting from blunt trauma. Endovascular techniques, including the use of self-expanding stents, are increasingly considered as options for managing vertebral artery dissection.
In this particular case, full anticoagulation therapy was not initiated due to the risk of secondary hemorrhage into the pathologically altered brain tissue [8]. Decompressive craniectomy as an anti-edematous procedure was not possible due to circulatory instability; stabilization of multiple organ failure was prioritized. In the case under study, the patient‘s demise, occurring six days subsequent to injury sustained from a fall and head impact against a fixed object, was notable for bilateral vertebral artery dissection. This finding was corroborated by imaging and further elucidated through autopsy examination and microscopy. The patient‘s prognosis was unfavorable due to bilateral involvement.
Traumatic dissections are most frequently encountered in scenarios involving falls, car accidents, or hanging [9]. Extracranial segments of vertebral arteries are particularly prone to dissection due to their increased mobility and close contact with bony structures. Bilateral vertebral artery dissection is rare, but prompt diagnosis, coupled with understanding the mechanism of injury, can make timely neurosurgical intervention possible (endovascular techniques such as the self-expanding stent) [10]. This case report highlights the importance of initial investigation into cervical spine and head injuries, particularly the risk of vertebral artery dissection, where symptoms of arterial involvement may mask those indicative of cervical spinal cord injury. The complex treatment of arterial injuries in spine trauma requires a case-by-case approach.
Key points: Cervical spinal cord injury may mask arterial injury. Symptoms of arterial injury may include headache, neck pain, nausea, vomiting, vertigo, and ataxia. Extracranial segments of vertebral arteries have close contact with bony structures and are prone to dissection due to their increased mobility. CT, CTA is used as a primary diagnostic technique for the diagnosis of vertebrobasilar insufficiency.
Conflict of interest
The authors declare no competing interests.
Zdroje
1. Goyal K, Sunny JT, Gillespie CS et al. A systematic review and meta-analysis of vertebral artery injury after cervical spine trauma. Global Spine J 2023; 14(4): 1356–1368. doi: 10.1177/21925682231209631.
2. Caicedo J, Ortiz López A, Cardozo A et al. Disección espontánea de la arteria vertebral, una causa de accidente cerebrovascular en el adulto joven. Reporte de caso. Acta Colombiana de Cuidado Intensivo 2018; 18(2): 122–126. doi: 10.1016/j.acci.2018.02.003.
3. Tinková M, Kasík J, Lacman J et al. Uzávěr bazilární tepny disekcí v souvislosti s manipulací krční páteře-kazuistika. Cesk Slov Neurol N 2011; 74/107(3): 348–352.
4. Schellinger PD, Schwab S, Krieger D et al. Masking of vertebral artery dissection by severe trauma to the cervical spine. Spine 2001; 26 : 314–319. doi: 10.1097/00007632-200102010-00019.
5. Bártková A, Krajíčková D. Potraumatická disekce vertebrální tepny. Neurol Praxi 2005; 4 : 217–219.
6. Kaiser R, Mencl L, Haninec P. Lehké mozkové poranění – intrakraniální komplikace a indikační kritéria pro CT vyšetření. Cesk Slov Neurol N 2011; 74 : 330–334.
7. Smyk DS, Herath JC. Delayed rupture of a vertebral artery laceration: a case report and challenges for the forensic pathologist. Forensic Sci Med Pathol 2018; 14 : 536–540. doi: 10.1007/s12024-018-9999-1.
8. Hall M, Cheng D, Cheng W et al. Antiplatelet versus anticoagulation for asymptomatic patients with vertebral artery injury during anterior cervical surgery-two case reports and review of literature. Brain Sci 2019; 28; 9(12): 345. doi: 10.3390/brainsci9120345.
9. Galtés I, Borondo JC, Cos M et al. Traumatic bilateral vertebral artery dissection. Forensic Sci Int 2012; 214: e12–e15. doi: 10.1016/j.forsciint.2011.07.005.
10. Leng S, Li W, Cai Y et al. The endovascular treatment strategies of cerebrovascular injuries in traumatic brain injury. Chin J Traumatol 2025; 28(2): 81–90. doi: 10.1016/j.cjtee.2025.01.001.
Štítky
Dětská neurologie Neurochirurgie NeurologieČlánek vyšel v časopise
Česká a slovenská neurologie a neurochirurgie

2025 Číslo 4
Nejčtenější v tomto čísle
- Brief cognitive tests for clinical practice
- Neuropsychiatric systemic lupus erythematosus – diagnosis and treatment
- Subclavian steal syndrome as a cause of a transient ischemic attack
- Diagnostics and management of patients with radiologically isolated syndrome