
Influencing factors for axial symptoms after modified expansive open-door laminoplasty
Faktory ovlivňující axiální příznaky po modifi kované expanzivní open-door laminoplastice
Cíl: Našim cílem bylo sledovat frekvenci výskytu axiálních příznaků (axial symptoms, AS) po modifikované expanzivní open-door laminoplastice (EOLP) a vyhodnotit faktory ovlivňující AS. Metody: Bylo vybráno 80 pacientů, kteří od května 2020 do května 2022 podstoupili modifikovanou EOLP. Pacienti byli sledováni 12 měsíců po operaci a rozděleni na skupinu s AS a skupinu bez AS. Byla zaznamenána jejich výchozí data. Faktory ovlivňující AS po modifikované EOLP byly zkoumány pomocí binární logistické regresní analýzy. Výsledky: Během 12měsíčního sledování po modifikované EOLP se AS vyskytly u 26 (32,5 %) z 80 případů. Ve skupině s AS byla předoperační míra komprese míchy (preoperative spinal cord compression rate, PSCR) vyšší než u skupiny bez AS, pooperační vzdálenost posunu míchy vzad byla delší a pooperační rozsah pohybu (range of motion, ROM) při meziobratlové flexi-extenzi byl statisticky signifikantně menší (p < 0,05). Rizikovými faktory pro AS po modifikované EOLP byly zvýšená PSCR a zvýšená pooperační vzdálenost posunu míchy vzad (poměr šancí [OR] > 1; p < 0,05) a ochranným faktorem byl zvýšený pooperační ROM při meziobratlové flexi-extenzi (OR < 1; p < 0,05). Závěr: PSCR, pooperační vzdálenost posunu míchy vzad a pooperační ROM při meziobratlové flexi-extenzi úzce souvisí s výskytem AS po modifikované EOLP.
Klíčová slova:
axiální symptom – expanzivní open-door laminoplastika – ovlivňující faktory – rozsah pohybu
Authors:
W. He; J. Pan
Published in:
Cesk Slov Neurol N 2024; 87(4): 264-268
Category:
Original Paper
doi:
https://doi.org/10.48095/cccsnn2024264
Overview
Aim: We aimed to observe the incidence of axial symptoms (AS) after modified expansive open - -door laminoplasty (EOLP), and to analyze the influencing factors for AS. Methods: Eighty patients undergoing modified EOLP from May 2020 to May 2022 were selected. They were followed up for 12 months after operation and divided into an AS group and a non-AS group. Their baseline data were recorded. The influencing factors for AS after modified EOLP were explored through binary logistic regression analysis. Results: During the 12-month follow-up after modified EOLP, AS occurred in 26 (32.5%) of the 80 cases. In the AS group, the preoperative spinal cord compression rate (PSCR) was higher than that of the non-AS group, the postoperative spinal cord posterior displacement distance was longer, and the postoperative intervertebral flexion-extension range of motion (ROM) was statistically significantly smaller (P < 0.05). Increased PSCR and increased postoperative spinal cord posterior displacement distance were risk factors for AS after modified EOLP (odds ratio [OR] > 1; P < 0.05), and elevated postoperative intervertebral flexion-extension ROM was a protective factor (OR < 1; P < 0.05). Conclusion: PSCR, postoperative spinal cord posterior displacement distance and postoperative intervertebral flexion-extension ROM are closely associated with the incidence of AS after modified EOLP.
Keywords:
range of motion – axial symptom – expansive open-door laminoplasty – infl uencing factor
Introduction
Modified expansive open-door laminoplasty (EOLP), as a common posterior cervical spine surgery, is mainly applied in the treatment of cervical spondylotic myelopathy such as ossification of posterior longitudinal ligament and spinal stenosis [1]. Following modified EOLP, the spinal cord injury of patients is relieved and the risk of postoperative complications is reduced through partial resection of the vertebral lamina on both ends and central laminoplasty [2]. However, axial symptoms (AS) still occur in some patients after modified EOLP. AS is a common complication of posterior cervical spine surgery, which can cause posterior cervical tenderness and muscle spasm, seriously affecting postoperative recovery and lowering the quality of life [3]. Therefore, it is necessary to investigate the influencing factors for the incidence of AS after modified EOLP. Logistic analysis is a generalized linear regression analysis model often used for data mining, so it is of great significance for exploring the risk factors for diseases [4].
Thus, the influencing factors for AS after modified EOLP were explored by logistic analysis in this study, aiming to provide novel insights into future prevention and treatment.

Patients and methods
General data
A total of 80 patients undergoing modified EOLP from May 2020 to May 2022 were selected as the subjects, including 45 males and 35 females. The mean age was (63.50 ± 3.07) years, ranging from 54 to 73 years. The body mass index was 21–28 kg/m2, with a mean of (24.50 ± 1.07) kg/m2. The duration of primary diseases was 13–23 months, with a mean of (18.05 ± 1.56) months. In terms of the primary diseases, there were 46 cases of cervical spinal stenosis, 25 cases of multi-segmental disc herniation and 9 cases of calcification of the posterior longitudinal ligament. As for underlying diseases, arterial hypertension occurred in 36 cases and diabetes mellitus in 7 cases. Besides, 26 cases had a smoking history and 42 cases had a drinking history.
The inclusion criteria were as follows:
1. patients diagnosed as cervical spinal stenosis, multi-segmental disc herniation and calcification of posterior longitudinal ligament by imaging examination;
2. those undergoing modified EOLP;
3. those with the symptoms of spinal cord compression before treatment and failed conservative treatment for 3 months or longer, all accompanied by various degrees of numbness and weakness in the limbs;
4. those undergoing surgery performed by the same group of surgeons;
5. those who and whose family members signed the informed consent form.
The exclusion criteria were as follows:
1. patients with a history of cervical spine surgery;
2. those with cervical deformity or instability;
3. those with cervical spinal cord injury caused by trauma or tumor;
4. those with inverted cervical curvature shown by X-ray examination;
5. those with a history of neck sprain or frozen shoulder;
6. those with a history of chronic pain before surgery, including neuralgia, headache and trigeminal neuralgia.
Surgical procedures
Modified EOLP was performed. Specifically, after general anesthesia, the patients were placed in a prone position with the head fixed using a Mayfield head frame (Mizuho Medical Group, Tokyo, Japan), followed by routine disinfection and draping. A cervical posterior median incision was made, the nuchal ligament was incised, and paravertebral muscles were separated under the periosteum on both sides of the spinous process to fully expose the C3 and C6 spinous processes. A bone slot was created at 2 mm of the inner margin of small joint on the open-door side where the symptoms were severe, while a V-shaped bone slot was created deep to the medial cortex of bone using a high-speed drill (Dentis Co., Ltd., Seoul, South Korea) on the hinge side. The door was opened using a 1 mm ultra-thin lamina rongeur (Synthes GmbH, Oberdorf, Switzerland). The operation was conducted based on preoperative MRI images. In the case of spinal cord compression at C2–3, the C3 lamina was completely excised and the C2–3 ligamentum flavum was cleared. In the case of no spinal cord compression, the C3 lamina was partly excised. Among those preoperatively with spinal cord compression at C6–7, the C6–7 ligamentum flavum was partly excised, the C7 vertebral dome was partly excised for undermining spinal canal decompression, and the C7 lamina was preserved intact. Next, the C4–6 laminae were lifted one by one towards the door axis side, and lifted while being separated if the adhesion was severe. The ligamentum flavum and adhesion zone at the edge of the vertebral lamina were removed, and the inner margin of facet joint was removed to fully expose the dural sac thorough decompression. Afterwards, a mini titanium plate (Syntec Scientific Corporation, Shenkang, China) was placed on the open-door side, and fixed on the vertebral lamina and lateral mass with screws. After the C4–6 spinous process was trimmed, the incision was sutured layer by layer. Following the surgery, the patients wore a cervical collar.
Diagnostic criteria for AS and grouping method
The patients were followed up for 12 months after operation by telephone call and outpatient review. According to the related diagnostic criteria [5], AS was defined as neck--shoulder pain or new-onset persistent pain dominated by neck pain 3 months after operation (which could not be explained by other reasons), lasting for ≥ 1 month, with a visual analog scale (VAS) score > 2 points [6]. The patients were divided into AS group and non-AS group according to the presence or absence of AS.
Baseline data
The baseline data of patients were collected, including sex (male/female), age (≥ 60 years, < 60 years), body mass index (≥ 24 kg/m2, < 24 kg/m2), type of primary diseases (cervical spinal stenosis, multi-segmental disc herniation, and calcification of the posterior longitudinal ligament), duration of primary diseases, preoperative neck-shoulder pain (Yes, No), intraoperative blood loss (> 100 mL, ≤ 100 mL), preoperative Japanese Orthopaedic Association (JOA) score (the patient‘s physical function was assessed using the JOA score before operation [7], and the higher the score [totally 29 points], the more severe the dysfunction), operation time, preoperative spinal cord compression rate (PSCR) (the ratio of the sagittal diameter of spinal cord compressed by herniated intervertebral disc and/or protruding osteophyte of the compressed segment to that of spinal canal in the same plane on the midsagittal T2-weighted image of the cervical spine), postoperative intervertebral flexion-extension range of motion (ROM), postoperative spinal cord posterior displacement distance, diabetes [random blood glucose ≥ 11.10 mmol/L (Yes, No) ], arterial hypertension [diastolic blood pressure ≥ 90 mmHg and/or systolic blood pressure ≥ 140 mmHg (Yes, No) ], smoking history (Yes, No), and drinking history (Yes, No).
Statistical analysis
SPSS25.0 software (IBM, Armonk, NY, USA) was used for statistical analysis. Measurement data were described by mean ± standard deviation (x − ± s), and intergroup comparisons were performed using the independent-samples t-test. Count data were described by percentage (%), and subjected to the c2 test. The influencing factors for AS after modified EOLP were explored through binary logistic regression analysis. P < 0.05 was considered statistically significant.
RESULTS
Incidence of AS after modified EOLP
During the 12-month follow-up after modified EOLP, AS occurred in 26 (32.5%) of 80 cases.
Baseline data of patients
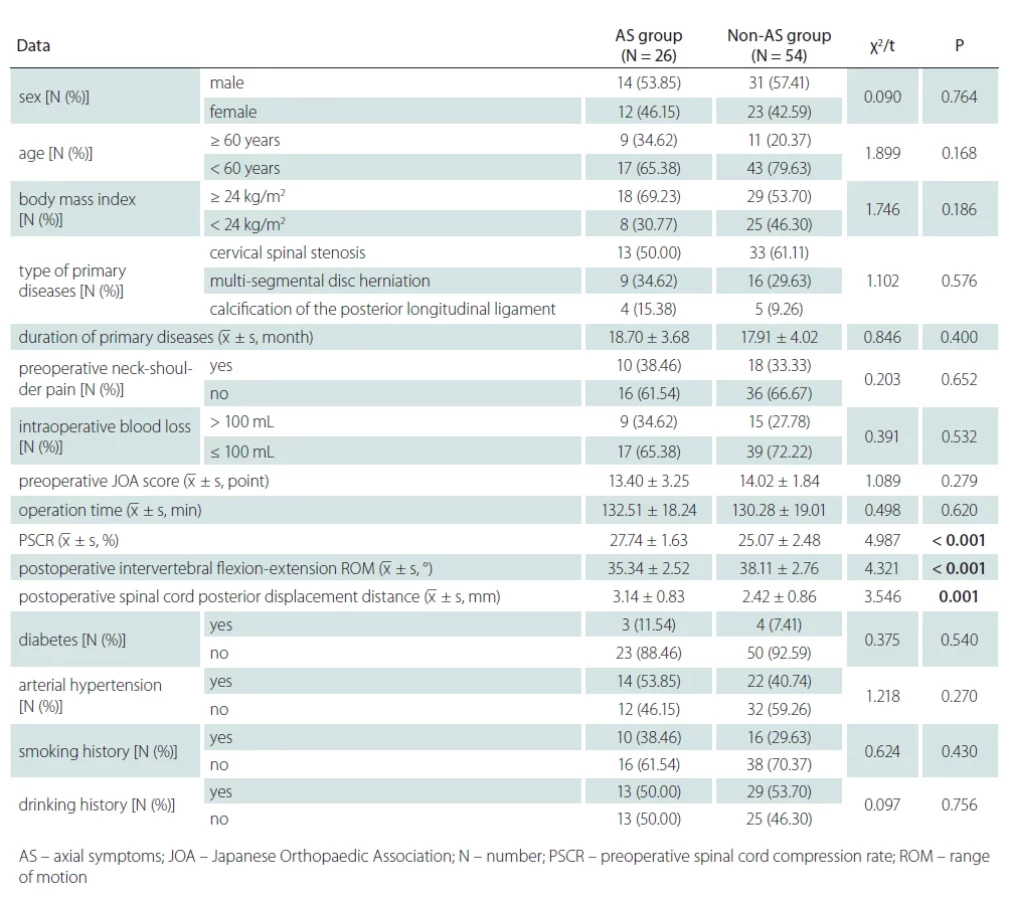
The AS group had a higher PSCR, longer post--operative spinal cord posterior displacement distance, and a smaller postoperative intervertebral flexion-extension ROM than those of the non-AS group (P < 0.05). No statistically significant difference was found in other data between the two groups (P > 0.05) (Tab. 1).
Results of binary logistic analysis of incidence of AS after modified EOLP
Simple logistic regression analysis was conducted, with the incidence of AS after modified EOLP as the dependent variable (“0” = AS, “1” = non-AS), and the statistically significant factors in Table 1 (PSCR, postoperative intervertebral flexion-extension ROM, and postoperative spinal cord posterior displacement distance) as the independent variables. Then the P value was set to < 0.1, and eligible factors were incorporated in binary logistic regression analysis. The results showed that increased PSCR and increased postoperative spinal cord posterior displacement distance were risk factors for AS after modified EOLP (OR >1; P < 0.05), while an increased postoperative intervertebral flexion-extension ROM was a protective factor (OR < 1; P < 0.05) (Tab. 2).
Discussion
Axial symptoms are mainly caused by factors such as destruction of the posterior cervical ligament complex, peeling off of C2 and C7 spinous process muscles, reduced mobility of the cervical spine, weakened neck strength, and local tissue adhesion and scar formation after cervical spine surgery [8]. Hunter et al. found that the incidence rate of AS after modified EOLP was 45–80% [9], higher than that (32.5%) in this study, which may be related to the difference between surgical skills. Compared to traditional posterior cervical expansive laminoplasty, modified EOLP can keep the vertebral stability, shorten the neck collar wearing time, promote rehabilitation and functional recovery shortly after surgery, and reduce the number of patients with postoperative axial pain, but AS may still occur [10]. Therefore, it is still necessary to find the factors related to the incidence of AS.
In this study, PSCR in the AS group was higher, the postoperative spinal cord posterior displacement distance was longer, and the postoperative intervertebral flexion--extension ROM was smaller than those of the non-AS group. The results of binary logistic regression analysis showed that increased PSCR and increased postoperative spinal cord posterior displacement distance were risk factors for AS after modified EOLP, while an increased postoperative intervertebral flexion-extension ROM was a protective factor.
The possible reasons are as follows. First, PSCR can reflect the overall status of anterior cervical spinal cord compression [11]. A higher PSCR means more evident posterior expansion of the dura mater following modified EOLP. During posterior expansion, the traction of the denticulate ligament and surrounding connecting structures against the spinal cord may be increased, thus causing cervical muscle tension and fatigue and inducing AS [12]. Meanwhile, the patients with a high PSCR suffer from greater pressure and obvious deformation of the cervical spinal cord, which can damage the vascular autonomic nerves innervated by the cervical spinal cord, induce local insufficient blood supply to the neck and shoulder, and lead to neck-shoulder pain and limited ROM, thus increasing the risk of AS [13]. Spinal cord ischemia-reperfusion injury may result from decompression following long-term compression, so the spinal cord undergoes congestion and edema, a large number of free radicals are generated, and inflammatory mediators are also secreted, thereby resulting in systemic inflammatory responses [14]. Ruan et al. also identified that increased PSCR was a significant risk factor for developing AS following EOLP [15].
Secondly, during modified EOLP, the posterior cervical ligamentous complex may be destroyed in the structure, and the posterior cervical muscles, nuchal ligament and posterior bony structure may be damaged, resulting in the loss of cervical ROM [16]. As a result, patients have weakened neck strength and long-term inability to move the neck, so local tissue adhesion and scar formation may occur after surgery, thus inducing AS [17,18]. Meanwhile, intervertebral controllability is weakened and the corresponding intervertebral torque and stress are concentrated due to decreased postoperative intervertebral flexion-extension ROM, so the degeneration of adjacent vertebrae that cannot tolerate shear or rotation is accelerated, and the risk of AS is increased [19]. Thus, more attention should be paid to the dynamic balance of cervical spine curvature and intervertebral flexion-extension ROM under postoperative physiological load. Intraoperative correction should not be overdone to obtain the static balance of cervical spine curvature and intervertebral flexion-extension ROM. Likewise, Lindenmann et al. reviewed the motion ranges and biomechanical impacts under physiological loads, which were crucial for maintaining both static and dynamic balance post-surgery [20].
Thirdly, excessive spinal cord posterior displacement may increase the traction against C4 and C5 cervical root in the bony fiber canal, then diminishing the function of cervical semispinalis muscles innervated by C4 and C5 cervical root [21]. The cervical semispinalis muscle is important for cervical stability, and it bears about 30% of the power for the function of cervical posterior extensors. In the case of function decline of the cervical semispinalis muscle, other posterior extensors begin to maintain the cervical dynamic stability in a compensatory way, so they are more prone to fatigue and injury, finally raising the risk of postoperative AS [22]. Therefore, a short distance (< 2 mm) of posterior displacement can provide enough space for relieving spinal cord compression. The main purpose of surgery is to obtain a satisfactory decompression effect, and there is no need to maximize the distance of posterior displacement. The patient‘s state should be fully assessed before surgery and closely observed after surgery to treat possible complications in a timely manner, thus reducing the risk of AS [23].
Conclusion
In conclusion, increased PSCR and increased postoperative spinal cord posterior displacement distance were risk factors for AS after modified EOLP, and elevated postoperative intervertebral flexion-extension ROM was a protective factor. Paying particular attention to these factors may help decrease the incidence rate of AS after modified EOLP.
Ethical principles
The entire study was conducted in accordance with the Helsinki Declaration of 1975 (as revised in 2004 and 2008). The study was approved by The First Affiliated Hospital of Soochow University (approval No. 2020-157) on May 5, 2020. Patients and there family members signed the informed consent form.
Conflicting interests
The authors declare they have no conflict of interest in relation to the subject of the study.
Sources
1. Nagoshi N, Nori S, Tsuji O et al. Surgical and functional outcomes of expansive open-door laminoplasty for patients with mild kyphotic cervical alignment. Neurospine 2021; 18 (4): 749–757. doi: 10.14245/ns.2142792.396.
2. Mo Z, Li D, Zhang R, Chang M et al. Comparison of three fixation modalities for unilateral open-door cervical laminoplasty: a systematic review and network meta-analysis. Neurosurg Rev 2020; 43 (3): 813–823. doi: 10.1007/s10143-018-1035-0.
3. Braun J, Kiltz U, Baraliakos X. Significance of structural changes in the sacroiliac joints of patients with axial spondyloarthritis detected by MRI related to patients symptoms and functioning. Ann Rheum Dis 2022; 81 (1): 11–14. doi: 10.1136/annrheumdis-2021-221406.
4. Eguchi Y, Suzuki M, Yamanaka H et al. Myovascular preserving open-door laminoplasty for cervical spondylotic myelopathy with miniplate fixation. Int J Spine Surg 2020; 14 (4): 476–482. doi: 10.14444/7062.
5. Poddubnyy D. Classification vs diagnostic criteria: the challenge of diagnosing axial spondyloarthritis. Rheumatology 2020; 59 (Suppl 4): iv6–iv17. doi: 10.1093/rheumatology/keaa250.
6. Sung YT, Wu JS. The Visual Analogue Scale for Rating, Ranking and Paired-Comparison (VAS-RRP): a new technique for psychological measurement. Behav Res Methods 2018; 50 (4): 1694–1715. doi: 10.3758/s13428-018-1041-8.
7. Li S, Kodama J, Wei L et al. Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire as an outcome measure for ossification of posterior longitudinal ligament patients in East Asia: an investigation of reliability, validity, and responsiveness. Ann Transl Med 2021; 9 (13): 1060. doi: 10.21037/atm-20-8064.
8. Ruan C, Jiang W, Lu W et al. Analysis of risk factors for axial symptoms after posterior cervical open-door laminoplasty. J Orthop Surg Res 2023; 18 (1): 954. doi: 10.1186/s13018-023-04426-9.
9. Hunter T, Sandoval D, Booth N et al. Comparing symptoms, treatment patterns, and quality of life of ankylosing spondylitis and non-radiographic axial spondyloarthritis patients in the USA: findings from a patient and rheumatologist Survey. Clin Rheumatol 2021; 40 (8): 3161–3167. doi: 10.1007/s10067-021-05642-6.
10. Cha JR, Kim HW, Yang DG et al. Open-door laminoplasty using lateral mass anchoring screws and non--absorbable sutures in patients with multilevel cervical myelopathy. Clin Orthop Surg 2020; 12 (4): 477–484. doi: 10.4055/cios20013.
11. Hou X, Lu S, Wang B et al. Morphologic characteristics of the deep cervical paraspinal muscles in patients with single-level cervical spondylotic myelopathy. World Neurosurg 2020; 134: e166–e171. doi: 10.1016/j.wneu.2019.09.162.
12. Nakashima H, Ishikawa Y, Kato F et al. Postoperative iatrogenic spinal cord herniation: three case reports with a literature review. Nagoya J Med Sci 2020; 82 (2): 383–389. doi: 10.18999/nagjms.82.2.383.
13. Nakajima H, Honjoh K, Watanabe S et al. Management of cervical spinal cord injury without major bone injury in adults. J Clin Med 2023; 12 (21): 6795. doi: 10.3390/jcm12216795.
14. Xue C, Ren P, Liang D et al. Surgical treatment of spinal thoracic metastases with nerve injury in patients with moderate-to-severe spinal cord injury. Ann Palliat Med 2020; 9 (5): 3204-3212. doi: 10.21037/apm-20-1507.
15. Ruan C, Jiang W, Lu W, et al. Analysis of risk factors for axial symptoms after posterior cervical open-door laminoplasty. J Orthop Surg Res 2023; 18 (1): 954. doi: 10.1186/s13018-023-04426-9.
16. Qu L, Li Z, Wang X et al. Axial symptoms after conventional and modified laminoplasty: a meta-analysis. World Neurosurg 2023; 180 : 112–122. doi: 10.1016/j.wneu.2023.09.086.
17. Ruspi ML, Palanca M, Cristofolini L et al. Digital Image Correlation (DIC) assessment of the non-linear response of the anterior longitudinal ligament of the spine during flexion and extension. Materials 2020; 13 (2): 384. doi: 10.3390/ma13020384.
18. Mörl F, Günther M, Riede JM et al. Loads distributed in vivo among vertebrae, muscles, spinal ligaments, and intervertebral discs in a passively flexed lumbar spine. Biomech Model Mechanobiol 2020; 19 (6): 2015–2047. doi: 10.1007/s10237-020-01322-7.
19. Zhou C, Li G, Wang C et al. In vivo intervertebral kinematics and disc deformations of the human cervical spine during walking. Med Eng Phys 2021; 87 : 63–72. doi: 10.1016/j.medengphy.2020.11.010.
20. Lindenmann S, Tsagkaris C, Farshad M, et al. Kinematics of the cervical spine under healthy and degenerative conditions: a systematic review. Ann Biomed Eng 2022; 50 (12): 1705–1733. doi: 10.1007/s10439-022-030 88-8.
21. Takahashi M, Iwamoto K, Tomita K et al. Incidence of cervical kyphosis and cervical posterior translation in neck pain associated with radiological evidence of degenerative disc disease. Musculoskelet Sci Pract 2022; 62 : 102637. doi: 10.1016/j.msksp.2022.102637.
22. Zhu XL, Xu WX, Ding WG et al. Analysis of influencing factors the postoperative axial symptoms of cervical single open-door laminoplasty. Zhongguo Gu Shang 2018; 31 (11): 1022–1026. doi: 10.3969/j.issn.1003-0034.2018.11.008.
23. Nardone R, Höller Y, Brigo F et al. The contribution of neurophysiology in the diagnosis and management of cervical spondylotic myelopathy: a review. Spinal Cord 2016; 54 (10): 756–766. doi: 10.1038/sc.2016.82.
Labels
Paediatric neurology Neurosurgery NeurologyArticle was published in
Czech and Slovak Neurology and Neurosurgery

2024 Issue 4
Most read in this issue
- Myastenie gravis – jak léčit pacienty co nejefektivněji?
- The Trail Walking Test to predict probable mild cognitive impairment in older adults
- Development of cognitive performance in children before and after surgical treatment of pharmacoresistant temporal lobe epilepsy
- Physical activity in people with multiple sclerosis and the impact of the COVID-19 pandemic